by Brenda Mahon, OTD, OTR/L, ATP
Many residents in long-term care environments spend a great deal of time seated in a wheelchair every day. Why do so many of them sit in poor postural alignment? Abnormal postures, although common, are treatable and can be prevented in many instances.
The following factors can contribute to abnormal postures:
- Poor wheelchair fit
- Inadequate equipment
- Fatigue
- Pursuit of postural stability
- Muscle tightness
- Impaired range of motion
One of the most significant hurdles clinicians face in long-term care is a limited selection of wheelchairs that will provide good postural alignment. Postural alignment is critical for independence in activities of daily living and mobility. Poor postural alignment and ill-fitting equipment can create long-term consequences that impact a person’s health and quality of life.
Poor, ill-fitting equipment may lead to:
- Increased fall risk
- Increased risk of pressure injury
- Impaired respiration
- Impaired swallowing
- Increased risk for aspiration
- Impaired digestion
- Decreased engagement/communication
- Impaired visual field
- Decreased socialization at risk for isolation and depression
- Increased risk for contractures
Posterior Pelvic Tilt

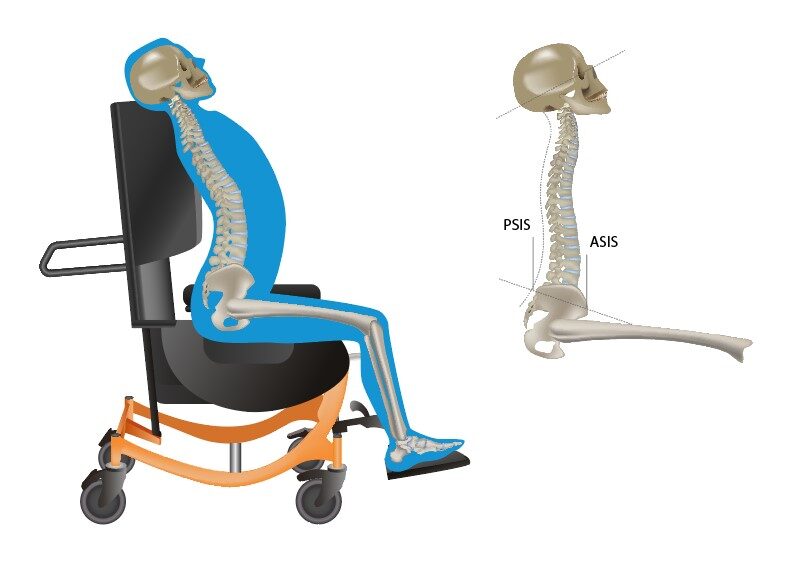
Posterior pelvic tilt is one of long-term care’s most prevalent postural abnormalities. The culprits are usually poor core strength/tone and tight hamstrings, resulting in a forward-flexed posture and a downward gaze.
A posterior pelvic tilt may increase difficulty breathing, interfere with digestion, increase pressure on the sacrum, increase pressure injury risk, and increase difficulty during transfers.
A posterior pelvic tilt can also inhibit heel strike, making self-propulsion difficult. We support the pelvis to prevent the pelvis from sliding forward.
Possible Interventions for Posterior Pelvic Tilt
Provide a cushion with a well for the sacrum and position the thighs with a slight abductor positioner.
If the wheelchair user has tight hamstrings, try to open the seat-to-back angle.
Don’t overlook the depth of the current seating system. Is the seat too long? Does the patient have limited hip flexion? A proper wheelchair seating assessment can help you determine if the wheelchair user is in the wrong size wheelchair.
Anterior Pelvic Tilt
Although not as common as a posterior pelvic tilt, anterior pelvic tilt can still cause problems for residents. Low tone, muscle weakness, or lordosis can be the causes of this issue. Possible consequences of this posture can include increased pressure on the pubis symphysis, increased risk of pressure injury, pain, and increased risk of falls.
Possible Interventions for Anterior Pelvic Tilt
A positioning belt across the anterior superior iliac spine (ASIS) can be helpful to mitigate an anterior pelvic tilt, although its use must be carefully documented. Used incorrectly, a pelvic belt may be considered a restraint, but if used for positioning purposes, the belt is acceptable for use in skilled nursing. Be sure to describe the clinical rationale when using a positioning belt thoroughly.
Pelvic Obliquity
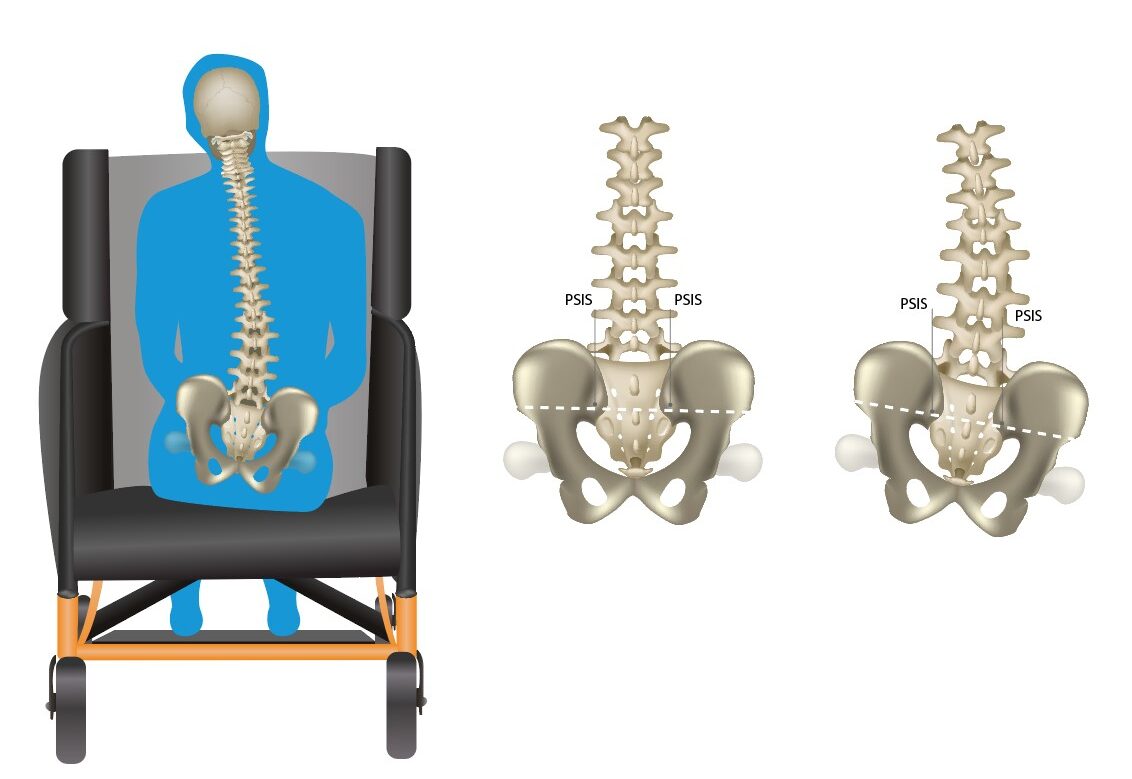
Pelvic obliquities can result from scoliosis or in individuals who have had hip surgery where the post-surgery side is higher than the other. Suppose the obliquity is not corrected or accommodated. In that case, it can increase the risk of pressure injuries since the pressure is concentrated on one ischial tuberosity and can lace pressure on the rib cage. If the obliquity is not corrected or accommodated, it can increase the risk of pressure injuries since the pressure is concentrated on one ischial tuberosity.
When a pelvic obliquity is suspected, always ensure the wheelchair user’s cushion is placed correctly and not causing the obliquity.
Possible Interventions for Pelvic Obliquity
If the obliquity is reducible, level the pelvis, building up cushioning under the lower side.
If the obliquity is non-reducible, accommodate for the deformity; raise the higher side.
Windswept Deformity

In windswept deformity, the pelvis has some rotation and/or an obliquity; one hip internally rotates and abducts, and the other externally rotates and abducts. The spine position will be dependent on the position of the pelvis. There is usually lateral flexion of the neck and may include forward flexion and rotation.
Possible Interventions for Windswept Deformity
Choose a cushion that is adjustable to accommodate the rotation or obliquity. Also, avoid using elevating leg supports on the patient’s wheelchair. The use of elevating leg supports may exacerbate the windswept posture.
Do you want to sit here?

Sling-seat wheelchairs are among the most common standard wheelchairs seen in skilled nursing facilities, but they may contribute to postural abnormalities. Sling seats cause internal hip rotation, and the lack of pelvic support will create a posterior pelvic tilt. This is especially true if the wheelchair is worn out and the seat is hammocked.
Did you know the sling-seat wheelchair model wasn’t designed for all-day use? In fact, it was originally intended to accommodate a 175 lb. man for only 1 hour. Our patients in skilled nursing facilities sit for many hours a day. A sling-seat or sling-back wheelchair would not be appropriate for most clients in skilled nursing facilities or long-term care settings. These wheelchairs are not only uncomfortable but do not provide support. If the patient is not already exhibiting postural abnormality, this wheelchair will likely cause the conditions we’d like to prevent. Using these basic wheelchairs sets the stage for pressure injuries, pelvic and spinal misalignments, and other expensive and painful pressure injuries. As clinicians, we can do better for our patients!
Have questions about seating and positioning for abnormal postures? Contact Broda’s seating and positioning experts for help at 844-552-7632 or by email at info@brodaseating.com.


